The new rules of heart health — Part 2 – What you should actually be measuring

In Part 1 of this series, we covered the Cardiovascular-Kidney-Metabolic (CKM) framework, which uses a holistic approach to risk assessment, as well as the new PREVENT cardiovascular risk calculator. This new calculator is an important step in the right direction because, as leading cardiologist Dr Mohit Gupta has recently published, Western cardiovascular risk calculators have historically missed 80% of heart attacks in Indian patients. In addition, the average age of a first heart attack amongst men in India is 54, whereas it is 65 for men and 72 for women in the US. In today’s blog post (#69) which is part 2 of this series, we go deeper into the numbers that actually tell you what’s going on. Most people who’ve had a blood test know their LDL-Cholesterol, which is the so-called “bad” cholesterol. But the 2026 guideline makes something clear: LDL-Cholesterol alone is not enough. There are at least three other numbers you should know, and several factors that can quietly push your risk higher without ever showing up in a standard test.
Before we get started, a quick note. Over the past two years, this blog has grown from a small experiment into a community of over 40,000 readers. The Longevity Circle WhatsApp group has also grown to more than 3,000 members. I’m deeply grateful for the trust this community has placed in us.
These efforts are supported by a small group of doctors and dietitians who generously contribute their time.
If you’ve found value in these posts or the community, and would like to support this work, you can do so by subscribing at $10 per month, $100 per year, or choose a Founding Pledge of $250 per year by clicking here (note the currency shows up in dollars irrespective of the country). There is absolutely no obligation. A heartfelt thank you to those who have already supported this effort.
I remain committed to keeping the community and the blog free and making trustworthy health advice actionable, accessible, and affordable for everyone.
Now back to our regular programming…
Beyond LDL-Cholesterol: The numbers that matter
LDL-C (aka LDL-Cholesterol is the more accurate way to represent the bad cholesterol but the term LDL is often used interchangeably and for the rest of the conversation I will stick to using the shorter LDL term) remains important, and the 2026 guideline sets specific targets based on your risk level:
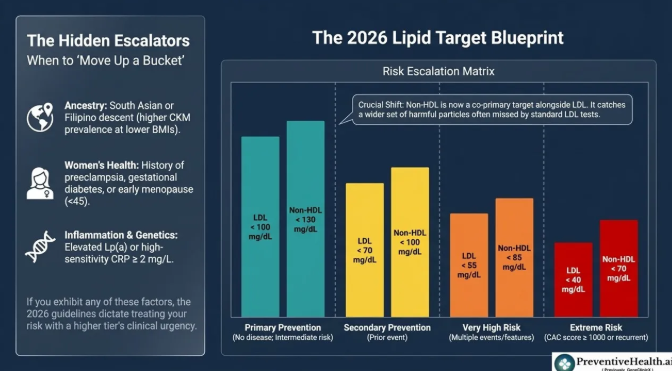

The calcium score (CAC) is used differently from the other factors in this table. In the first three rows, risk is determined by your overall profile, including your history, blood tests, and risk calculator, so CAC is not recommended by the guidelines to define those categories. The last row is different because an extremely high CAC score (≥1000) directly reflects a very high plaque burden and can by itself define the “extreme risk” category.
Notice that every row has two targets, not one. That brings us to the first of the three numbers most people don’t know about.
Non-HDL cholesterol: The number already in your results
Non-HDL cholesterol is simply your total cholesterol minus your HDL. Your lab already calculates it automatically; it’s right there in your results, but often ignored.
Why does it matter? Because LDL only measures the cholesterol in LDL particles in your blood. Non-HDL catches a wider set of harmful particles, including those that carry triglycerides (a type of fat in your blood). In people with diabetes, obesity, or elevated triglycerides, LDL can look fine while non-HDL remains elevated, which means your real risk is higher than LDL alone suggests.
The 2026 guideline elevates non-HDL to a co-primary target alongside LDL for the first time. So make sure to look at that number more closely.
ApoB: The most precise measure of particle risk
The second of the three numbers is one I have covered in a past blog post: Apolipoprotein B (ApoB) directly counts the number of harmful cholesterol particles in your blood, not just how much cholesterol they’re carrying. Think of it as counting the trucks on the highway, not just estimating the cargo.
The guideline recommends testing ApoB particularly if you:
- Have already hit your LDL and non-HDL targets for your risk level, but have diabetes, elevated triglycerides, or CKM syndrome (i.e., being in Stage 1 or higher of the Cardiovascular-Kidney-Metabolic framework).
- Have low LDL (below 70 mg/dL) but still have residual risk of a heart attack. Residual risk is the risk that remains even when LDL is low, driven by factors like inflammation, genetics, or metabolic issues.
In these situations, LDL can appear controlled while ApoB remains high, meaning the particle count is elevated even if the cholesterol mass looks acceptable. ApoB surfaces that hidden risk.
Lp(a): The test that’s slowly beginning to gain attention
The last of the three is also one I have covered in a previous blog post: Lipoprotein(a), written as Lp(a) and pronounced “LP little a”. It is a cholesterol particle that behaves a lot like LDL but with an added inflammatory component. Roughly 1 in 5 people carry elevated levels of it. Most have never been tested.
Here is why the 2026 guideline makes testing Lp(a) a Class I recommendation (its strongest) for all adults at least once in their lifetime:
- Lp(a) is almost entirely genetically determined; diet and exercise don’t meaningfully change it, and neither do standard statins
- Levels at or above 50 mg/dL affect about 20% of the population and are linked to roughly 40% higher cardiovascular risk
- Levels at or above 100 mg/dL roughly double your risk
- Very high levels (~180 mg/dL) carry a risk comparable to familial hypercholesterolemia, a serious inherited cholesterol disorder, thereby more than tripling your cardiovascular disease risk
- People of South Asian or Latin American ancestry face higher population-level heart attack risk from elevated Lp(a) specifically
If your Lp(a) is high, the current response is to manage every other controllable risk factor more aggressively. Dedicated Lp(a)-lowering therapies are in late-stage clinical trials and likely to become available in the coming years.
Factors that quietly raise your risk
The 2026 guideline has a formal list of risk enhancers: factors that should push your doctor toward treating you more aggressively, even if your calculated risk score seems borderline. These don’t change the calculator output, but they should change the conversation.
From your family history:
- A parent or sibling who had a heart attack or stroke before age 55 (men) or 65 (women)
From your blood tests:
- Elevated Lp(a)
- High-sensitivity CRP ≥ 2 mg/L on more than one test — a marker of systemic inflammation
- Triglycerides persistently ≥ 150 mg/dL fasting, or ≥ 175 mg/dL non-fasting
- LDL persistently 160–189 mg/dL despite lifestyle efforts
From your health history:
- Type 2 diabetes or CKM syndrome
- Chronic inflammatory conditions: e.g. rheumatoid arthritis, lupus, or severe psoriasis
For women specifically, which is often missed:
- Preeclampsia, gestational hypertension, gestational diabetes, or preterm delivery during a past pregnancy
- Early menopause (before age 45)
Women who experienced any of these, carry meaningfully higher long-term cardiovascular risk. These are now officially listed in the guideline’s risk-enhancer table, but they are often overlooked in women’s routine care. If any of these apply to you, bring them up with your doctor explicitly.
On ancestry: While the 2026 guideline has removed race from its risk equations entirely, South Asian and Filipino ancestry remain listed as official risk enhancers in the clinical decision table. South Asian individuals have higher rates of diabetes at lower BMI, higher Lp(a)-associated cardiovascular risk, and higher CKM syndrome prevalence. If this applies to you, your ancestry should factor into the “Personalize” step of the CPR framework (Calculate → Personalize → Respond), even though the calculator itself doesn’t use it.
A simple way to apply this is to ‘move up a bucket’: if you are of South Asian or Filipino descent and your calculator result is Borderline, you should treat it with the clinical urgency of an Intermediate risk and consider starting a statin or ordering a Calcium Scan immediately.
A simple doctor’s visit checklist
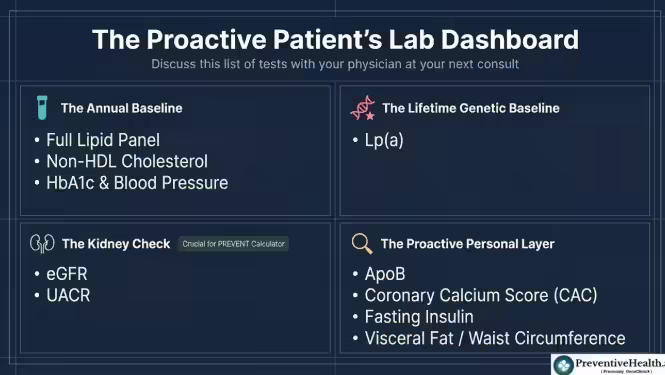
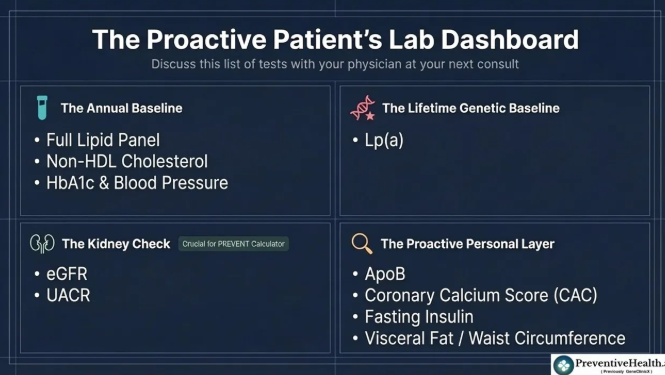
Here are the tests the 2026 guideline supports requesting. Most routine checkups miss several of these:
Standard (should be in every annual check):
- Full lipid panel — total cholesterol, LDL, HDL, triglycerides
- Non-HDL cholesterol — already in your results, just make sure to review it
- HbA1c (average blood sugar)
- Blood pressure
Kidney function (needed to run the PREVENT calculator):
- Serum creatinine → used to calculate eGFR (unless EGFR shows up on your blood report)
- Urine Albumin-to-Creatinine Ratio (UACR) — catches early kidney stress even when eGFR looks normal
Once in your lifetime:
- Lp(a) — Class I guideline recommendation for all adults
If you have diabetes, elevated triglycerides, or CKM syndrome:
My personal recommendations (not from the guidelines):
- I find fasting insulin useful for detecting insulin resistance before HbA1c rises. This isn’t a standard guideline recommendation, but it’s worth discussing with your doctor if you have a family history of diabetes or metabolic issues.
- I also suggest getting your ApoB measured proactively, irrespective of whether you have diabetes, elevated triglycerides or CKM syndrome.
- For individuals of South Asian or Filipino ancestry, where risk may be underestimated, a calcium scan should be considered earlier and used more proactively to guide decisions.
- Finally, I highly recommend measuring your visceral fat or waist circumference because the thin-fat Indian (TFI) is a real thing. I know because I was one…..BMI 23 and visceral fat 12
The bottom line from part 2
Standard cholesterol tests tell you part of the story. Non-HDL, ApoB, and Lp(a) complete it. And several risk factors, including pregnancy history, early menopause, inflammation markers, visceral fat, and ancestry, can significantly change your risk picture without ever showing up in a routine check.
In Part 3, we’ll cover lifestyle: what the guidelines actually say about diet, exercise, weight, and supplements, including which “heart health” products the guideline explicitly says don’t work.
As always, I welcome your thoughts and would love to hear your experiences in the comments.
Nickhil Jakatdar is the CEO of GenePath Diagnostics and the founder of PreventiveHealth.ai, working to make advanced diagnostics and credible health guidance more accessible, affordable, and actionable. A PhD in EECS from UC Berkeley and the youngest recipient of the UC Berkeley Distinguished Alumnus Award, he has founded and led multiple tech companies. He holds 60 patents, and serves on several academic, healthcare, and innovation boards. To follow his thinking on preventive health, technology, and systems that scale expertise, join his private WhatsApp community and subscribe to his Substack.
Disclaimer
Views expressed above are the author’s own.
END OF ARTICLE